


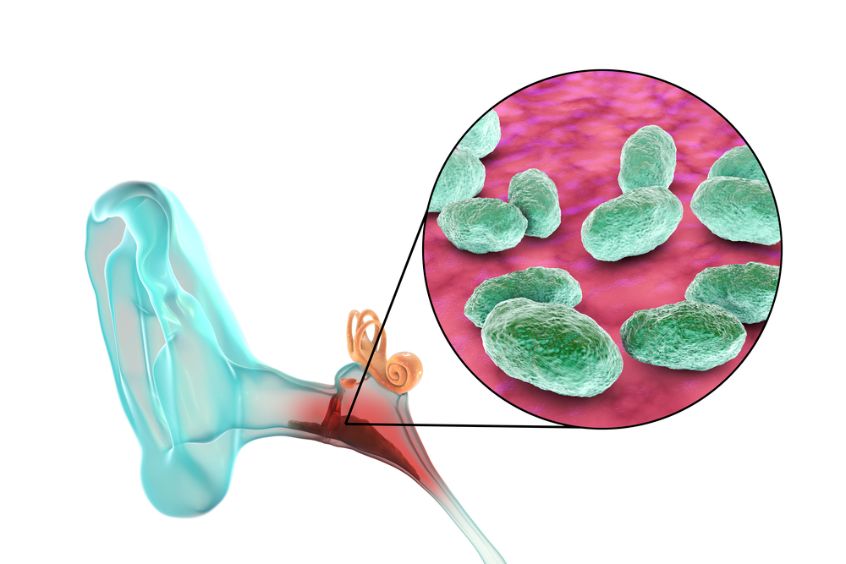
Acute otitis media is a common childhood infection caused by a bacteria or virus. This disease can cause ear pain and a fever. Children may also have irritability, headache, and disturbed sleep. They may also have poor feeding, anorexia, vomiting, or diarrhea.
Infections of the middle ear occur most commonly between 3 months and 3 years of age, as the eustachian tube is immature and less flexible in this age range. The eardrum, a thin, smooth bone that separates the outer and inner ear, is fragile and can easily tear in an acute otitis media infection.
The bacterial infections that lead to acute otitis media can spread into the surrounding tissue or into the brain, causing mastoiditis (infection of the bony protrusion behind the ear) or petrositis (inflammation of the tympanic membrane). In some rare cases, a severe bacterial middle ear infection can even cause a hole in the eardrum and a brain abscess.
Treatment for acute otitis media includes antibiotics, which are most effective in children under 2 years of age and those with mild symptoms. High-dose amoxicillin is the most common antibiotic used for this condition.
If the symptoms do not improve after 48 to 72 hours of antibiotic treatment, a second course of antibiotics may be needed. It is important to complete the full course of antibiotic therapy, as a repeat infection may occur if a new virus or bacteria mutates and becomes resistant to the first medication.
Old-fashioned remedies such as a warm water bottle or bag of salt can help relieve ear discomfort. However, they are not helpful in hastening the clearing of the middle ear fluid and should not be used for any longer than necessary.
Symptoms of chronic otitis media include hearing loss and persistent drainage from the middle ear, eardrum, or mastoid (rounded bone behind the ear). The hearing losses associated with chronic otitis media can affect speech and language development in young children.
Risk factors for otitis media include being exposed to second-hand cigarette smoke and having a family history of recurrent ear infections. Exposure to other children in group settings such as day care centers and preschools increases the risk of otitis media. Using a humidifier can help alleviate symptoms in children with acute otitis media.
Other problems can result from recurrent or persistent otitis media, including chronic perforation of the eardrum and changes in the bones and cartilage of the ear. These changes can lead to bone erosion, bone spurs, eardrum attenuation, or damage to the ossicular (bone) structure of the middle ear.
The risk of facial paralysis can be increased by a history of recurrent or chronic otitis media in a child younger than 24 months. This can be due to anatomic abnormalities, inadequate antibiotic treatment, or a particularly virulent pathogen that penetrates the eardrum and spreads into the facial nerve.
Acute otitis media is often the first sign of an upper respiratory tract infection, which makes it difficult to diagnose without an ear exam and a throat culture. Laboratory tests, such as strep or pneumonia cultures and blood tests for viral markers, are sometimes needed to confirm the diagnosis.






{kind=link}